The Division of Head and Neck Oncology provides a comprehensive center for the diagnosis, work up and management of benign and malignant disorders of the thyroid and parathyroid glands, including in-office ultrasound guided fine needle aspiration, molecular testing of thyroid nodules through Thyroseq, and state of the art imaging, such as 4-Dimensional CT scan for parathyroid disease.
Our surgeons collaborate with radiologist, oncologists, pathologists and endocrinologist, discussing and managing patients in a multidisciplinary fashion at the weekly UNC Head and Neck Tumor Board and our monthly UNC Endocrinology Tumor Board.
Our thyroid cancer patients our managed by a treatment group of surgeons, endocrinologists, nutritionists and radiologists, who provide education on low-iodine diet, surgical management, thyroid hormone withdrawal versus thyrogen stimulation for radioactive iodine treatment, counseling from radiation safety in preparation to iodine treatment, as well as long-term surveillance with standard of care imaging and work.
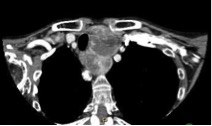
Enlarged thyroid glands, particularly those that expand under the breast bone(sternum) and collar bone(clavicle) may cause compression of the airway and esophagus leading to difficulty breathing and swallowing, particularly when patients lay flat.
Total Thyroidectomy is a cost effective alternative to medical therapy and radioactive iodine for the management of patients with over active thyroid glands/nodules (low TSH – thyroid stimulating hormone; elevated Free T4 – circulating thyroid hormone), and is particularly useful in medically-refractory cases or when there is concern for malignancy. Outpatient surgery is performed in selected cases.
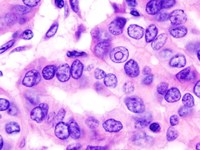
Papillary and Follicular Thyroid Cancer are the most common forms of thyroid cancer, and the incidence has been increasing. The local control and survival for the majority of patients is excellent with surgery with or without post operative iodine therapy, and in skilled hands, such as those of the UNC surgical group, the risks of life alter voice dysfunction, swallowing dysfunction and calcium dysfunction is low (<1%). Early stage cancers may be managed with a drainless outpatient procedure.
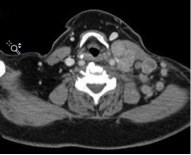
A significant portion of thyroid cancer patients (roughly 50%) have either occult (not radiographically visible), visible or recurrent disease in the lymph nodes around the thyroid in the central compartment or within the lateral neck around the great vessels. With the unparalleled experienced of managing a variety of head and neck malignancies, our head and neck surgeons are extremely facile in the management of neck disease.
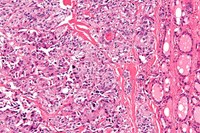
A lower incident, more aggressive form of thyroid cancer, medullary thyroid cancer may be sporadic (seen in a individual) or hereditary (within a familial) and associated with genetic mutations and associated disorders. Patient receive comprehensive laboratory and imaging work up, as well as genetic testing and counseling when appropriate, prior to surgery.
Previously presumed to be uniformly fatal and managed with palliative radiation therapy, growing evidence in the literature suggests that some patients may benefit from heroic surgical resection, which our surgeons perform in select cases.
A technique for surgical removal of parathyroid disease or low-volume thyroid disease through a 1.5-2 cm midline neck incision with the use of endoscopes for visualization.
The use of robotic surgery for management of thyroid disease is optimally suited for patients with unilateral indeterminate thyroid nodules, in an otherwise normal-sized thyroid lobe, who wish to undergoing hemithyroidectomy without a neck incision. The techniques involved an 8-10 cm incision in the axilla (armpit) or a similar length incision starting behind the ear and extending down the hairline.
Hyperparathyroidism may be due to a solitary adenoma (over-active parathyroid gland), hyperplasia (over-activity of all 4 parathyroid glands) , and may be a consequence of renal failure. The condition disturbs the body metabolism, specifically a patients calcium metabolism, which can affect multiple organ systems. Pre operative work up includes, laboratory testing, such as PTH (parathyroid hormone) level testing, imaging studies, such as sestamibi, technetium and 4D CT scans. The surgery is typically an outpatient procedure and may be performed with MIVAT techniques.