
The approach to treating kidney tumors should always be personalized based on the patient’s needs, but a recent publication by UNC Urologist Marc Bjurlin, DO, MSc and NYU Physicians Stella Kang, MD, MSc and William C. Huang, MD suggest expanding the recommendations set forth by the American Urological Association for treating small benign-appearing kidney tumors.
Recognizing the low risk of developing metastatic disease from small lesions, the 2017 American Urological Association guidelines for treating kidney tumors recommend that patients with very small lesions (<2 cm) can undergo active surveillance rather than primary surgical treatment.
This course of action can be difficult to communicate to patients as it requires an understanding of low-level, cancer-specific mortality risk for lesions of this size and in the absence of medical comorbidities, patients could be provided the option of pursuing a biopsy.
Kidney tumors containing enhancing soft tissue on CT or MRI that do not have features typically observed in benign tumors should be considered malignant unless proven otherwise— as 75-80% of such lesions are ultimately confirmed to be malignant. In the past, because the malignant potential for small kidney tumors was unknown, they were usually resected. This is not an ideal approach as the other 20-25% of patients with benign lesions wouldn’t have required surgical intervention. Further, many of the patients with malignant lesions didn’t metastasize while under observation.
Metastatic disease rates are currently only 1-2% in reported observational studies over 2 to 3 years and The Delayed Intervention and Surveillance for Small Renal Masses registry for all small kidney tumors <= to 4 cm support that these tumors are generally indolent; all patients who started with active surveillance had a 100% cancer-specific survival rate of over 5 years.
In support, patients presenting with small kidney tumors are usually 60 years old or older when diagnosed and often have substantial comorbidities. Due to this, these patients have increased mortality after a kidney tumor resection, further favoring active surveillance.
“Given the natural history of localized kidney cancers, the long-term benefit of treatment, particularly in older adults with multiple medical comorbidities, depends in large part on competing risks of death. With this in mind, risk assessment remains key in the counseling and management of patients with small renal masses.”
Dr. Marc Bjurlin
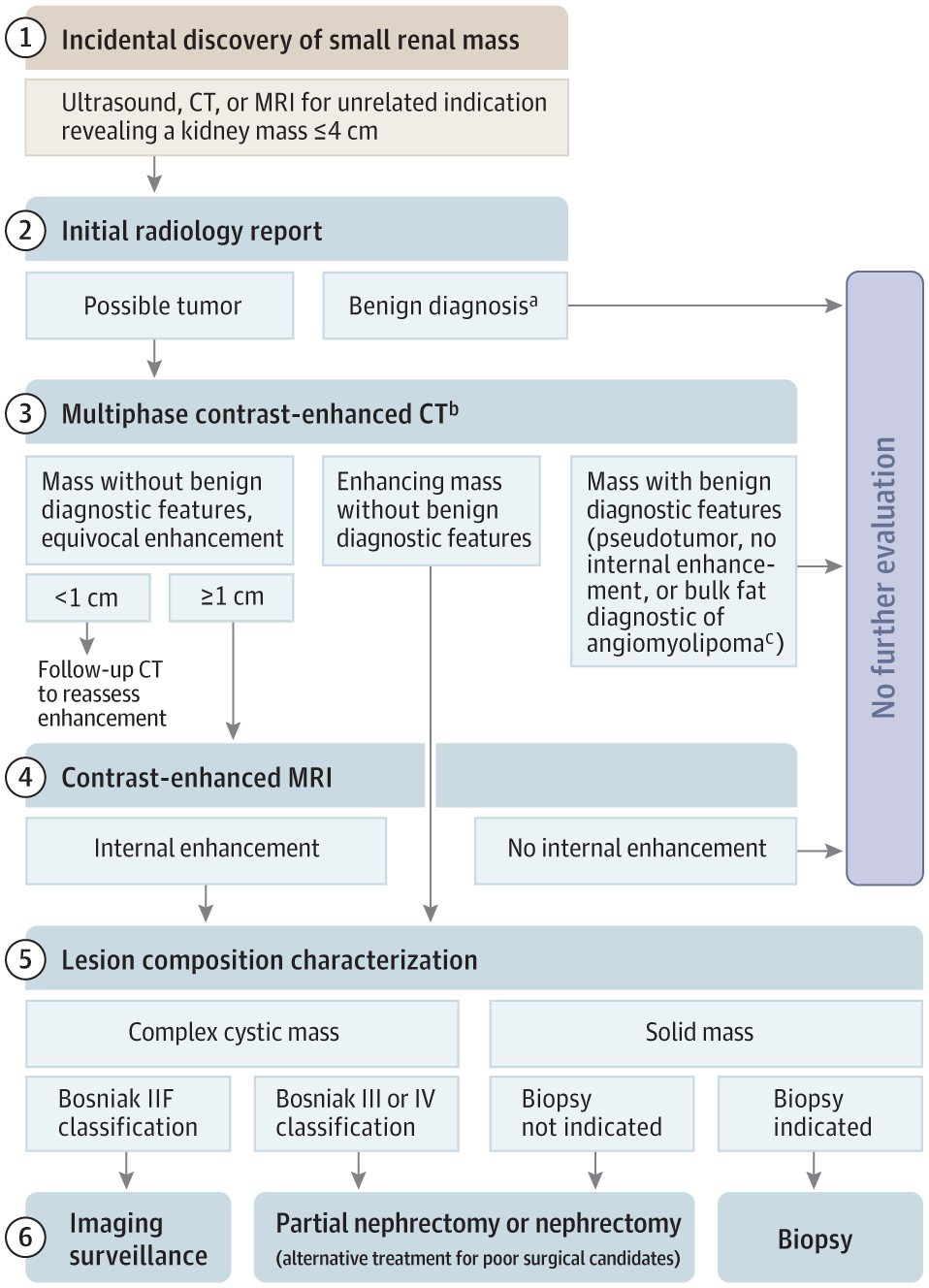
Considered Approaches to Diagnosis and Management of Small Kidney Tumors
a) Benign diagnoses can be made from the appearance alone for a number of lesions including simple cysts (Bosniak I), cysts with few uniformly fine septa or fine calcification (Bosniak II), pseudotumors, focal pyelonephritis, vascular lesions, and kidney infarction.
b) Magnetic resonance imaging (MRI) with contrast may be preferred to computed tomography (CT) in patients with moderate or severe decreases in kidney function or history of severe allergic reactions to iodinated intravenous contrast agents.
c) For centrally located tumors consider renal sinus lipomatosis. Angiomyolipomas >3 cm may need follow-up imaging to monitor growth.
Read The Full Publication at JAMA
Citation:
Kang SK, Bjurlin MA, Huang WC. Management of Small Kidney Tumors in 2019. JAMA. Published online April 01, 2019. doi:10.1001/jama.2019.1672