Decoding the ANA: A guide to ANA testing
The Antinuclear Antibody test, or ANA, is a blood test that can help diagnose autoimmune diseases like lupus. ANAs can bind and damage certain structures within a cell’s nucleus. The ANA test is frequently misunderstood. This website can help you decide when to order an ANA, counsel your patient about the test, and interpret ANA test results.
ANA testing is one piece of information that may help you diagnose an autoimmune disease like systemic lupus erythematosus. The ANA should only be ordered after a careful clinical evaluation uncovers clinical features of concern for an autoimmune disease. This includes a thorough history and physical exam and sometimes basic labs such as a blood count, chemistry, and urine tests.
- An ANA should be ordered if you have a high suspicion for an autoimmune disease such as Sjogren’s, Lupus, or Scleroderma. (See table below.)
- ANA is NOT recommended in patients with isolated fatigue, back pain, headaches, non-specific musculoskeletal pain, paresthesia, abdominal pain, or vague symptoms such as diffuse pain.
Table 1: Autoimmune diseases associated with a positive ANA:
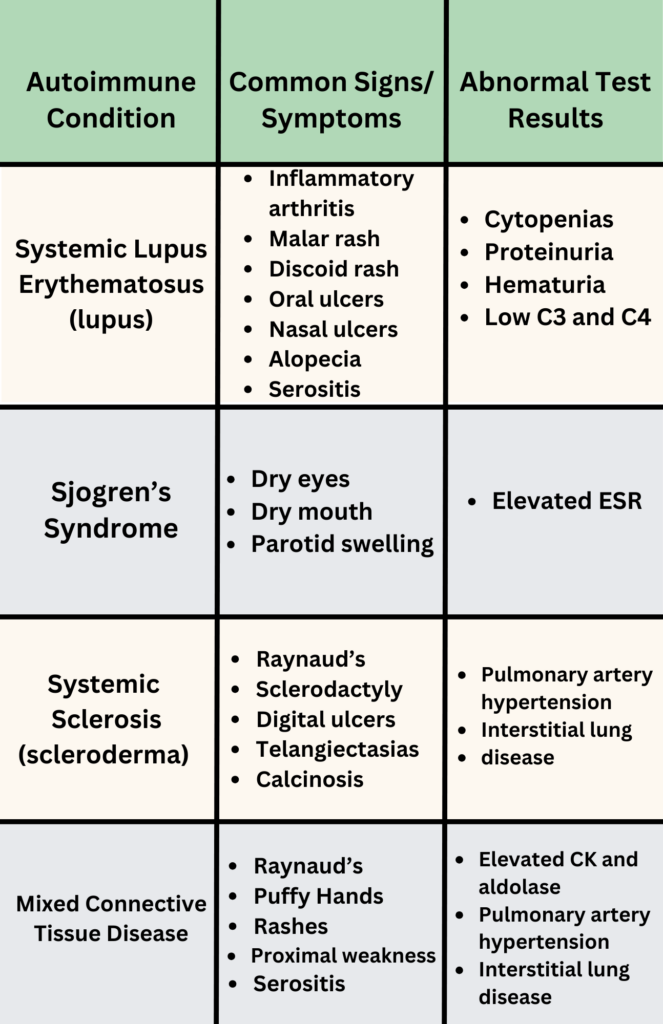
- A positive ANA does NOT need to be repeated! 2
- A positive ANA only indicates antibodies are present. It does NOT mean a patient has an autoimmune disease.
- If positive, additional testing for antigen specific antibodies should only be considered if presentation is consistent with an autoimmune disease.
- Serial ANA tests in autoimmune disease is NOT useful to monitor disease activity. The ANA will usually still be positive even when an autoimmune disease is well controlled.
- A negative ANA does NOT need to be repeated!
- If the ANA test is negative, do not order additional antibody testing.
- If an autoimmune disease such as lupus is suspected, more lab tests can be helpful. Consider checking the following:
- CBC with differential
- CMP
- Urinalysis and Urine Protein/Creatinine ratio
- dsDNA
- Extractable nuclear antigen (ENA)
- C3 and C4 complements
Very carefully! A positive test does NOT diagnose an autoimmune disease! Positive ANA can be seen in up to 20% of healthy adults. ANAs are not specific and can be seen in several autoimmune diseases. ANA can also be positive in other conditions including infections (e.g., tuberculosis, endocarditis, HIV, Hepatitis C, EBV), malignancy, and lymphoproliferative disorders.
The level at which the sample is diluted with a recognizable stain is the ANA titer. The clinical significance of ANA titers can be difficult to assess. Up to 30% of healthy individuals have a positive ANA of 1:40 or greater. Higher ANA titers are more likely to be clinically significant. In one study analyzing ANA titers in patients with confirmed autoimmune diseases, the median ANA titer was 1:320.
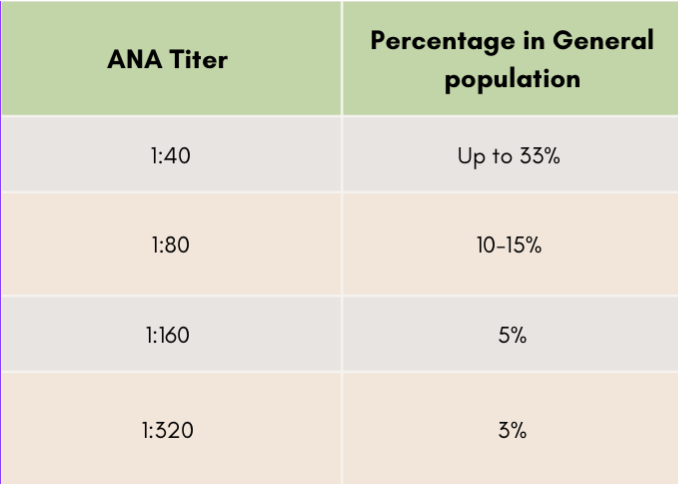
As you can see, low titer ANA antibodies are found frequently in the general population. Even high titer ANA’s can be seen in healthy adults who do not have an autoimmune disease.
Counseling a patient with a positive ANA can be challenging since this result can often be misinterpreted. Patients need you to guide them through the next steps. It is important to let a patient know that the positive result only indicates an antibody is present. Emphasize that a positive test result can also be seen in healthy individuals. A positive ANA test alone does NOT diagnose a specific autoimmune disease. Sometimes further investigation is indicated if there are symptoms suggestive of an autoimmune disease.
Patients need to know that a positive test result can also be seen in healthy individuals.
Sometimes further testing or consultation with a rheumatologist can be helpful. Patients with a positive ANA who do not have symptoms of an autoimmune disease do NOT need to see a rheumatologist.
If there is low concern for an autoimmune condition, it is important to address the patient’s fears and anxieties while providing reassurance that a positive test result does not mean the patient has a new diagnosis.
Healthcare costs continue to rise. ANA screening can have a high background positivity rate in the general population. When ANA is checked for vague symptoms, it can lead to misdiagnosis, additional testing, and unnecessary referral to rheumatology. In a retrospective study, less than 10% of patients referred to an academic rheumatology clinic for a positive ANA had an ANA-associated rheumatic disease.[i] Inappropriate ANA testing places a strain on healthcare resources and undue anxiety for patients.
- Consider ordering an ANA if a patient has signs or symptoms of lupus, Sjogren’s, or scleroderma.
- An ANA should not be ordered for headaches, diffuse pain, back pain, isolated fatigue, or vague complaints without other signs or symptoms.
- A positive ANA is not sufficient for diagnosing lupus or other autoimmune diseases.
- 20% of healthy adults have a positive ANA.
- If an ANA is positive, it should be interpreted using the context of specific symptoms and clinical findings (i.e., skin tightening, lupus rashes, inflammatory arthritis, oral or nasal ulcers, alopecia, cytopenia, etc.).
- Patients with a positive ANA who do not have symptoms of an autoimmune disease do NOT need to see a rheumatologist.
- Only check additional antibodies if the ANA is positive AND the patient has signs or symptoms of an autoimmune disease.
- Do NOT repeat an ANA test.
Kumar, Bhatia, and Minz, “Antinuclear Antibodies and Their Detection Methods in Diagnosis of Connective Tissue Diseases.”
Kavanaugh et al., “Guidelines for Clinical Use of the Antinuclear Antibody Test and Tests for Specific Autoantibodies to Nuclear Antigens.”
Wei et al., “Analysis of Antinuclear Antibody Titers and Patterns by Using HEp‐2 and Primate Liver Tissue Substrate Indirect Immunofluorescence Assay in Patients with Systemic Autoimmune Rheumatic Diseases.”
Tan et al., “Range of Antinuclear Antibodies in ‘Healthy’ Individuals.”
Abeles and Abeles, “The Clinical Utility of a Positive Antinuclear Antibody Test Result.”
Narain et al., “Diagnostic Accuracy for Lupus and Other Systemic Autoimmune Diseases in the Community Setting.”