In this age of technology, it’s not unheard of to be wearing 3D printed earrings or shoes, using 3D printed measuring cups in the kitchen or gracing your dining room table with 3D printed plates and cups. Today, 3D printed items can be found almost everywhere…even in the operating room. The use of these items in the medical field has its place, as was the case with a 3D model of the human heart that helped a surgeon work through the intricacies of his latest surgery on a patient with a rare congenital heart defect.
Deanna Williams was a 27-year-old mother of two, pregnant with her third child, a ticking time bomb. She had no idea she had been born with a rare congenital heart defect and that her pregnancy could unexpectedly put too much pressure on her heart leading to possibly fatal consequences. Luckily, however, her story takes a much different path.
At four months pregnant, Deanna began to experience symptoms unrelated to her growing child. “Every time I ate, it felt like someone was sitting on my chest,” says Deanna. “My heart would race so badly that I eventually ended up in the emergency room. They couldn’t do any extensive tests until after my daughter was born, but they referred me to a cardiologist, Dr. Richard Pacca, who put me on beta blockers to prevent heart failure and heart attacks.”
During her pregnancy, because doctors had determined something was going on with her heart, Deanna was unable to do some of the most basic tasks, including picking up her children and holding them in her arms. She was on limited activities, no exercise and no lifting anything over 10 pounds. “I was always on edge about what I could and couldn’t do,” Deanna explains. “The bigger I got, the more pressure it became. It got so bad at one point that I couldn’t even hold my purse because it felt so heavy on my chest.”
Once her child was born, doctors started the process of finding out exactly what was happening with Deanna’s heart. Her cardiologist, Dr. Richard Pacca, ordered extensive testing including MRIs and CT Scans which helped him to figure out what was going on with her heart. He referred her to UNC Medical Center in Chapel Hill so they could help clarify the picture with more advanced technology. She was eventually diagnosed with Anomalous Aortic Origin of the Coronary Artery (AAOCA). It is a rare birth defect in which the coronary artery is connected at the wrong location on the aorta. This complication can cause a decrease in blood flow to the heart tissue referred to as ischemia and lead to sudden death in otherwise healthy individuals.
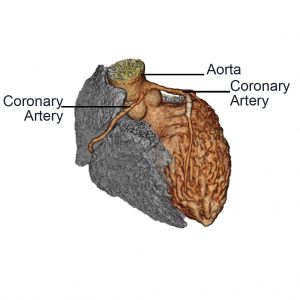
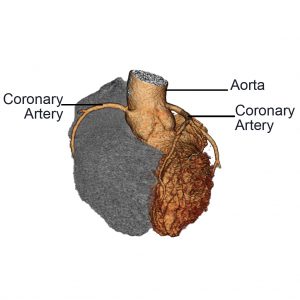 Normal Anatomy of the Coronary Arteries Normal Anatomy of the Coronary Arteries |
 Anomalous Aortic Origin Anomalous Aortic Originof the Coronary Artery (AAOCA) |
To explain AAOCA further, the coronary arteries are vessels that arise from the aorta (the biggest vessel in the body) and provide blood supply to the heart. There are usually two: the left and right coronary arteries. The coronary arteries flow from one of three locations on the aorta called sinuses of Valsalva. The right coronary artery comes off the right sinus of Valsalva and the left coronary artery from the left sinus. With the diagnosis of AAOCA, the coronary artery is flowing from the incorrect sinus of Valsalva; for example, the left coronary artery is coming from the right sinus.
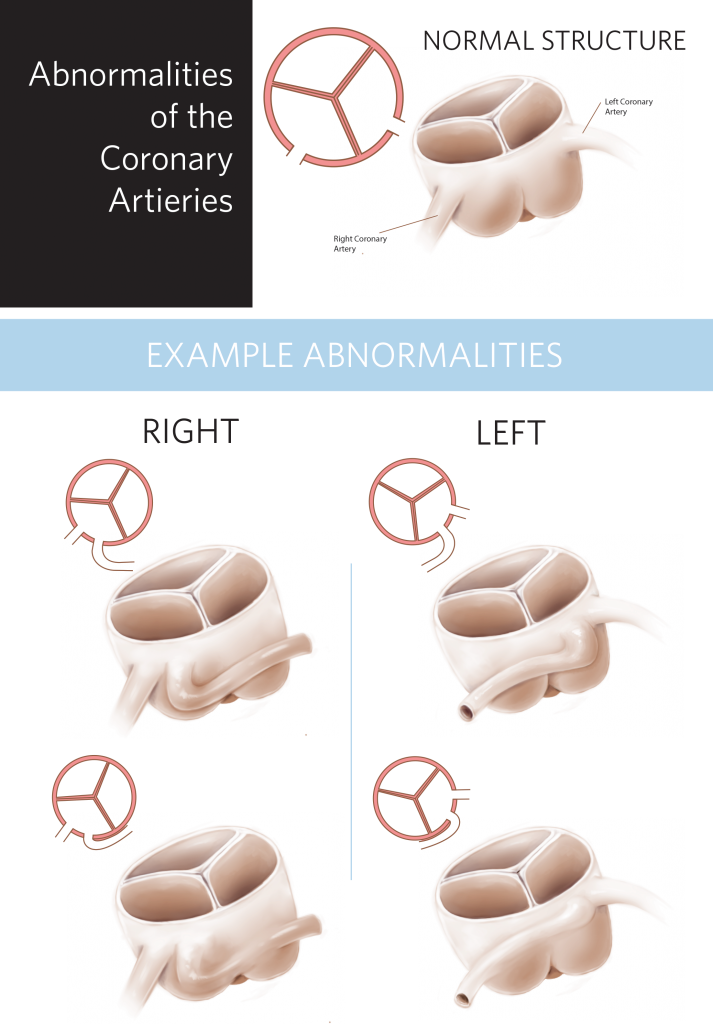
“With AAOCA,” notes Dr. Mahesh Sharma, Co-director of the NC Children’s Heart Center and Section Chief of Congenital Cardiac Surgery at UNC Medical Center, “there are multiple factors associated with this birth defect. Factor one, in Deanna William’s case, her right coronary artery was coming from the left sinus of Valsalva. Factor two, that same coronary artery was running in the wall of the aorta, which is called intramural coronary artery. Factor three, when the coronary artery comes from an incorrect side of the aorta, it means that the artery has to take a different path to the heart. Deanna’s artery was running between the two great arteries, the aorta, and the artery to the lungs, the pulmonary artery, which is called intra-arterial. So anytime she did any exercise which enlarges the pulmonary artery, it was putting pressure and pinching the coronary artery, restricting blood supply, because it wasn’t where it was supposed to be.”
The final factor for Deanna was not uncovered until Dr. Sharma reached out to Dr. Brian Hyslop, Radiologist and head of the 3D imaging lab at UNC Medical Center. Within the last year, Dr. Hyslop and his team, including Andrew Woodward, 3D Imaging Technologist, started offering 3D services to doctors across UNC Health Care.
“Dr. Sharma reached out to us because he knew his patient had a congenital anomaly of the coronary artery,” says Dr. Hyslop, “but wanted to be able to visualize it better, to better understand the relationship of the two vessels that were flowing from the aorta to the heart. He was also interested in being able to see the interior of the vessel, and we could help him do that.”
Using their software, Andrew not only created a 3D printed model of the heart for Dr. Sharma but he also allowed Dr. Sharma to conduct what they call a fly through, actually allowing him to visually walk through the vessels on the screen, so he knew what to expect before Deanna’s surgery. “Using the CT scan which provides us volumetric data and measurements,” says Andrew, “I can create a 3D image on the screen. Imagine peeling an apple in one long segment. When you put it all back together, you have the whole apple, but when you stretch it out, it’s like a slinky. You have a slinky of data that you put into the software from the 2D CT scan and on the screen shows up the heart and vessels. We can surf through a particular vessel, see some of the branches left or branches right, up or down, see if it narrows or widens, and so on.”
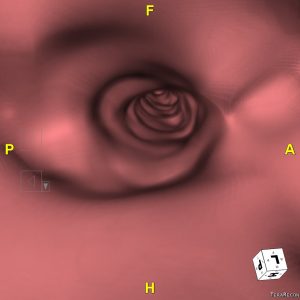

During the fly through process, Dr. Sharma came upon the fourth and final factor associated with this particular form of AAOCA for Deanna Williams. When doing the fly through Dr. Sharma noticed that the opening inside of the aorta, which should be round, allowing easy flow of blood, was compressed into a slit. Due to the multiple factors associated with her heart defect, doctors agreed that the best course of action would be surgery.
On November 8, 2018, Deanna underwent surgery to correct her congenital heart issues. Once her recovery period was complete, she could once again pick up her children, carry her purse and continue to live her life. Deanna could have been another statistic, another unfortunate person born with an undiagnosed heart defect that was taken from the world too early, leaving behind a family of loved ones. With the help of the team at UNC, Deanna has a much different story with a little 3D printed heart to prove it.
“Everybody at UNC was great, especially my surgeons and anesthesia team,” says Deanna. “They made it a more bearable experience. They helped me get peace of mind about the whole situation. I do want to say special thanks to God, my loving supportive husband Barron, my kids Malaysia, Maliah and Mallorie. To all family and friends that prayed for me and helped out with taking care of the kids during this process.”