Rapid Response Guide

Flow of a rapid response:
- Introduce yourself and your role loudly
- Stand at the foot of the bed
- Eyeball patient quickly – ABC’s, if unresponsive ask if there is a pulse
- Intro Timeout
- Team introductions – roles and names
- Primary nurse sign out (SBAR: Situation, Background, Assessment, Recommendation)
- Interventions
- Determine disposition
- Debrief with the team
- Identify one learning point
Trouble shooting:
- Diagnostic pause and shared mental model – helpful once situation has been ongoing or if you feel stuck
- Review what you are thinking and what interventions have been done
- Think out loud
- Ask team: is there anything else?
- Closed loop communication
- Call for backup if needed – you can always call MICU, hospitalist on call, pharmacy, etc.
- If tenuous – assign someone to keep a finger on the pulse
- Use the Rapid Response ordersets created by Amanda Tosi
Rapid Response Scenarios
Atrial Fibrillation- Irregularly irregular rhythm
- Narrow complex UNLESS has repolarization abnormality — can see AFib RVR with aberrancy. Compare to prior ECGs to assess for this. If in doubt, assume wide complex rhythm is not supraventricular.
- Starling curve — too little or too much fluid
- ACS
- Sepsis
- PE
- Sympathetic surge (surgery, sepsis, hyperthyroidism)
- Electrolyte abnormalities
- IV metoprolol 5 mg up to 3x — contraindicated in severe lung disease
- IV diltiazem 10 mg up to 3x — contraindicated in HFrEF
- IV amiodarone 150mg over 10 minutes, followed by drip. Can take some time to work. Side effects include acute hypotension. Can cause stroke if converts to sinus rhythm and patient not anticoagulated.
- Esmolol drip (0.5 mg/kg IV over 1 minute load, then 0.05 mg/kg/min)— has to be reconstituted by pharmacy, can only give in certain hospital units.
- Synchronized cardioversion (120-200 Joules) — if unstable or refractory to above. Can consult cardiology to help with this, but if unstable should not delay. Consider versed (1-2 mg)/fentanyl (25-50 mcg) prior to administering if still responsive, should not delay in an emergent situation.
- Volume overload
- Acute flash pulmonary edema (hypertensive urgency, ACS, valvular disease)
- PE
- Aspiration
- Pneumothorax
- Pneumonia (typically more subacute)
- Pleural effusion (typically more subacute)
- Respiratory depression (narcotic overdose, acute stroke, seizure)
- Nitroglycerin paste (0.5 inch)
- Nitroglycerin drip (starting dose 5 mcg/min) — typically want an arterial line in place
- Furosemide, bumetanide, torsemide — depends on diuretic tolerance of patient and renal function
- CRRT/HD
Afterload reduction: arterial dilation
- Labetalol (20mg IV)
- Hydralazine (10mg IV) — least preferred, less predictable, can have significant hypotension leading to stroke or acute MI, especially with carotid stenosis, CAD
- Nitroprusside drop (starting dose: 0.25-0.5 mcg/kg/min) — typically want an arterial line in place

- Mnemonic (adopted from The Clinical Problem Solvers):

- Initial workup: based on your suspicion re: most etiologies, but you will never be wrong to obtain:
- POCT glucose
- CBC/differential
- CMP + Mg/Phos
- VBG/ABG
- Troponin + ECG
- Urinalysis
- Urine toxicology, serum ethanol
- Medication review (sedating medications or medication changes that raise risk for withdrawal/overdose)
- Bladder scan
- Additional workup: depending on risk factors/exam, consider:
- AM cortisol
- INR/PT, APTT
- Abdominal x-ray
- Chest x-ray
- CT head non-contrast
- Vitamin B12, RPR, TSH, HIV
- Lumbar puncture
- Continuous EEG
- Urine pregnancy test
- Neurology consult
Background:
- Risk factors: increasing age, hypertension, and systemic anticoagulation/antiplatelets
- Presentation: headache, vomiting, altered mental status/stupor/coma, seizures, hypertension
Workup:
- Laboratory: POCT glucose, CBC/diff, CMP, PT/INT, APTT, troponin, urinalysis, urine toxicology, urine pregnancy
- Imaging: STAT non-contrasted head CT, ECG
Initial management:
- ABC stabilization
- Code BAT
- Neurosurgery consult
- Control blood pressure:
- Goal: If SBP 150-220 mmHg, goal = 140 mmHg within 1 hour; If SBP >220, goal = 140-160 mmHg over several hours
- Labetalol 20 mg IV – repeat as necessary
- Nicardipine infusion – start at 5 mg/mL, titrate to goal SBP (max 15 mg/mL)
- Reverse anticoagulation: *Use UNCHCS Anticoagulation Reversal Order Panel + call your pharmacist*
- Warfarin: KCentra (Prothrombin complex) preferred over FFP + phytonadione (vitamin K) 10mg IV
- Heparin/Enoxaparin: IV protamine
- Dabigatran: idarucizumab (Praxbind)
- Apixaban, Rivaroxaban: coagulation factor Xa (Andexxa) or Kcentra
-
Fondaparinux, Bivalirudin, Argatroban: Kcentra
- Manage increased intracranial pressure (if present): consider if mass effect or edema on imaging, concern for herniation, or Cushing triad (bradycardia, respiratory depression, HTN)
- Prevention: head of bed at 30 degrees, mild sedation if agitation, treat fever, position head straight without IJ lines/tight trach ties/etc., isotonic fluids ONLY, serum Na >135 mEq/L
- Treatment:
- Hypertonic saline (23.4%) 15-30 mL IV bolus over 10 minutes – needs central line
- Mannitol (20% infusion) 0.5-1 g/kg IV once (contraindicated in anuria or pulmonary edema)
After initial management:
- Transfer to higher level of care (typically under neurology or neurosurgical service in the NSICU)
- Q1 neuro checks
- BP and sodium goals – per neurology/neurosurgery and critical care teams
Reverse anticoagulation: *Use UNCHCS Anticoagulation Reversal Order Panel + call your pharmacist*
-
- Warfarin: KCentra (Prothrombin complex) preferred over FFP + phytonadione (vitamin K) 10mg IV
- Heparin/Enoxaparin: IV protamine
- Dabigatran: idarucizumab (Praxbind)
- Apixaban, Rivaroxaban: coagulation factor Xa (Andexxa) or Kcentra
- Fondaparinux, Bivalirudin, Argatroban: Kcentra
Seizure > 5 minutes or multiple seizures without return to baseline level of consciousness
Stabilization – should be FIRST step while beginning to consider etiology/diagnostics
- Start timing!
- Airway/breathing/circulation (ABCs)
- Place on 100% oxygen and cardiorespiratory monitoring
- Consider a nasopharyngeal airway
- If unable to oxygenate or protect airway, early Rapid Sequence Intubation (RSI)
- Obtain IV/IO access
- Place on 100% oxygen and cardiorespiratory monitoring
- 1st line therapy: benzodiazepine
- Lorazepam (Ativan) 0.1 mg/kg to max 4 mg IV/IO
- Diazepam (Valium) 0.2 mg/kg to max 10 mg IV/IO (may repeat once)
- Midazolam (Versed) 0.2 mg/kg to max 10 mg IV/IO (may repeat once)
- If NO IV/IO access:
- Midazolam (Versed) 10mg IM x1 (5 mg if 13-40 kg)
- Midazolam (Versed) 10 mg intranasal spray
- 2nd line therapy: Antiseizure medication
- Levetiracetam (Keppra): most commonly 1000 mg (60 mg/kg to max 4500 mg IV/IO)
- Fosphenytoin: use fosphenytoin order panel for dose by weight (most commonly 1500 mg IV if >62.5 kg)
- Phenytoin 20 mg/kg IV/IO – preferred only if fosphenytoin unavailable or administering via IO
- Valproate 40 mg /kg to max 3000 mg
- STAT Neurology consult
- Consider transfer to higher level of care with additional imaging (MRI, cvEEG) and studies (lumbar puncture) depending on risk factors
Diagnostics:
- POCT glucose
- CBC/differential
- CMP + Mg/Phos
- Urinalysis
- Urine toxicology
- Serum levels of any home seizure medications
- Urine pregnancy test
- STAT CT head non-contrast
Etiologies to consider:
- Lowered seizure threshold due to acute illness
- Electrolyte derangements
- Hypoglycemia
- Alcohol or benzodiazepine withdrawal/cocaine or amphetamine intoxication
- Stroke/trauma
- Posterior reversible encephalopathy syndrome (PRES) (especially if hypertensive)
- Eclampsia (if pregnant)
- Intracranial infection (meningitis, encephalitis, abscess
- Mnemonic: ACUTE ABDOMEN (a proposed POCUS protocol for ED evaluation of acute abdominal pain)
- Abdominal aortic aneurysm
- Collapsed inferior vena cava (volume status)
- Ulcer with perforated viscus
- Trauma (free fluid)
- Ectopic pregnancy
- Appendicitis
- Biliary tract
- Distended bowel loop (obstruction)
- Obstructive uropathy
- MEN – testicular torsion / Women – ovarian torsion
- Physical exam: A quick “Does the patient need the OR?” evaluation

- Initial workup: based on your suspicion re: most etiologies, but you will never be wrong to obtain:
-
- CBC/diff
- CMP
- Lipase
- Lactate
- VBG/ABG
- UA
- Urine pregnancy
- Troponin
- X-ray – supine vs upright vs left lateral decubitus
- ECG
- CT– with contrast versus AAA protocol versus mesenteric ischemia protocol
- POCUS
Initial management:
- ABC stabilization
- Obtain access
- Fluid resuscitate
- Make NPO / confirm last PO intake
- Hold anticoagulation / reverse anticoagulation if needed
After initial management:
- Pain / nausea control – do not delay for surgical evaluation (data proves that opiates do not obscure the diagnosis)
- Obtain labs and imaging
- Place blood products on hold if you anticipate significant bleeding (PRBCs, FFP, platelets)
- Insert NG tube, on suction if concern for obstruction
- Start antibiotics if concern for perforated viscus or infection (zosyn, meropenem, cipro/flagyl)
- Consult surgery STAT – use buzz words: peritonitic, rigid, elevated lactate, free air
- Transfer to higher level of care (typically transfer to surgery service if going to the OR)
UGI Bleed

Stabilization – should be FIRST step while beginning to consider etiology/diagnostics:
- Establish access (2 large bore IVs – 16 gauge or cordis)
- Fluid resuscitation
- Transfuse (if patient is actively bleeding with reasonable concern, you should transfuse immediately and do not need to wait for labs)
- Consult Gastroenterology vs VIR
Diagnostics:
- Endoscopy is first choice and typically preferred within 24 hours, for non-variceal bleeding, and perhaps within 12 hours for variceal bleeding.
- CT angiography can detect active bleeding and provide a target for VIR particularly
- Consider patient’s stability when planning for a CT scan
Medications:
Administer appropriate medications as indicated by patient scenario and comorbidities
- IV PPI for acid suppression and prevention of further erosion
- Pantoprazole 80 mg IV bolus x1, then 40 mg IV BID
- Prokinetics to improve gastric visualization (Erythromycin or Metoclopramide) [rarely given]
- Vasoactive medications variceal bleeding (Somatostatin)
- Octreotide drip: 100 mcg bolus x1, then 50 mcg/hour infusion
- Antibiotics for upper GI bleed in cirrhosis
- Ceftriaxone 1g IV daily (preferred over fluoroquinolone) – goal to administer prior to endoscopy
- TXA: Deemed to not be an effective treatment for GI bleeding. Administered in this given concern for oropharyngeal bleeding.
Don’t forget to hold antihypertensives and anticoagulants
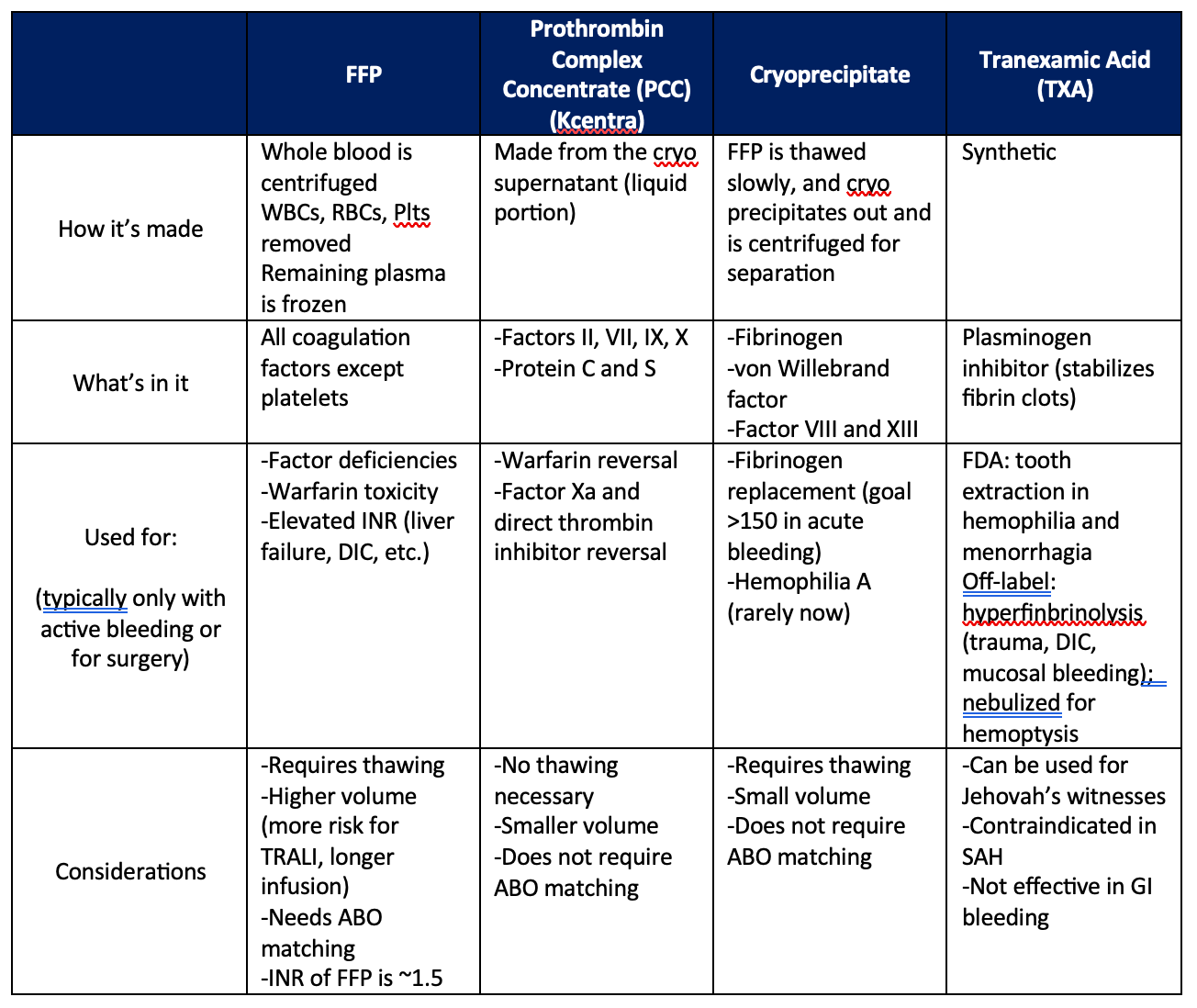
Transfusion protocol:
Massive transfusion protocol:
- Activated by making a phone call to the blood bank
- First round: 6 units of PRBCs, 6 units of FFP, and 1 unit of platelets
- Second round: 6 units of PRBCs, 6 units of FFP, and 1 unit of cryoprecipitate
- If patient does not have type and screen, you can activate emergency blood by filling out a pink slip to administer uncross-matched blood
- Trend CBC [RBCs, platelets], PT/INR, PTT [FFP], and fibrinogen [cryoprecipitate]
- Goal Hgb >7, Platelets >50, INR 1.5, fibrinogen >150 or evaluation via thromboelastogram (Qstat)