Imagine: You have a patient with a penicillin allergy documented in their chart. Typically, you would prescribe amoxicillin for their infection, but that is not an option because it is a penicillin-class antibiotic. Instead, you prescribe a broader-spectrum antibiotic–not your first choice except for the allergy. But, what if you learned that it is not a true allergy?
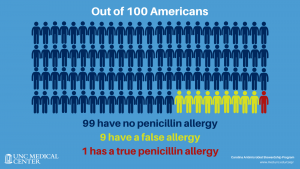 Less than one in ten patients in the US with a reported allergy to penicillin are truly allergic. It is not uncommon for an allergy to disappear over time or for an allergy to be documented incorrectly. When a healthcare provider sees a penicillin allergy in a patient’s medical record, they may prescribe a beta-lactam alternative that could have a broader spectrum. Use of these alternative antibiotics is associated with more side effects, higher healthcare costs for both patients and facilities, and antimicrobial resistance.
Less than one in ten patients in the US with a reported allergy to penicillin are truly allergic. It is not uncommon for an allergy to disappear over time or for an allergy to be documented incorrectly. When a healthcare provider sees a penicillin allergy in a patient’s medical record, they may prescribe a beta-lactam alternative that could have a broader spectrum. Use of these alternative antibiotics is associated with more side effects, higher healthcare costs for both patients and facilities, and antimicrobial resistance.
The allergy is removed, or “de-labeled”, from a patient’s medical record after an evaluation shows the patient is no longer allergic. A recent study conducted in the UNC Medical Center Emergency Department found that nearly one in four patients (24%) had their penicillin allergies de-labeled after assessment by a trained pharmacist. De-labeling makes penicillin-class drugs such as penicillin, amoxicillin, Augmentin, ampicillin, and Zosyn, among others, an option for treating common infections in the future, which many experts agree is often the best course of action.
“With more than 240,000 patients in the UNC Health System with a documented penicillin allergy, there is ample opportunity to expand assessments,” explained Renae Boerneke, PharmD, CPP, BCPS, who co-leads a project to encourage penicillin allergy assessment with Mildred Kwan, MD, PhD. Since assessments started in 2020, project partners assessed more than 80 patients in outpatient areas; more than 30 patients had their allergies de-labeled.
In 2020, Boerneke and Kwan were recognized as Improvement Scholars by the University of North Carolina at Chapel Hill’s Institute for Healthcare Quality Improvement (IHQI). As IHQI’s project support comes to a close this month, the expansion of allergy assessments to inpatients will continue under the auspices of UNC Medical Center’s Carolina Antimicrobial Stewardship Program.
Earlier this year, the team created a penicillin allergy assessment tool kit to educate patients and train healthcare providers to proactively assess penicillin allergies. Boerneke is currently recruiting pharmacists to participate in offering assessments in both inpatient and outpatient areas [learn more].

Donna Krzastek, PharmD, MPH, BCPS, was among the first pharmacists to say yes. “One way to approach the public health problem of antimicrobial resistance is by building strong stewardship practices,” she said. Krzastek noted that patients with a documented penicillin allergy are more likely to have higher rates of multidrug-resistant organisms and a greater likelihood of an adverse drug reaction.
“I believe penicillin allergy assessments improve the overall quality of care for our patients. They also have a positive impact on our workplace culture by expanding opportunities to be actively involved in antimicrobial stewardship,” she continued. “After learning more about the project from Dr. Boerneke, I knew I wanted to be a part of the expansion to inpatients at Hillsborough Hospital.”