Building models of integrated, trauma-informed prenatal care for pregnant women with substance use disorders takes time and collaboration. And, it’s a worthy task that could save the lives of women and children and stop harmful cycles for healthier generations.
A new paper from UNC Horizons’ Director of Health Services Elisabeth Johnson, PhD, NP, outlines the current opioid crisis and the specific needs of women within that crisis. “Models of care for opioid dependent pregnant women” was published in the March 2019 issue of Seminars in Perinatology.
 Opioid use disorders continue to grow in the United States, with more than 115 deaths related to opioid overdose every day. This national crisis impacts women the most, with deaths from prescription opioid overdose increasing at rates that are alarmingly high compared to men. Pregnant women with opioid use disorders face what may feel like insurmountable barriers to accessing proper prenatal care, accessing substance use disorder treatment options, lack of insurance coverage, legal consequences, stigma, trauma and more.
Opioid use disorders continue to grow in the United States, with more than 115 deaths related to opioid overdose every day. This national crisis impacts women the most, with deaths from prescription opioid overdose increasing at rates that are alarmingly high compared to men. Pregnant women with opioid use disorders face what may feel like insurmountable barriers to accessing proper prenatal care, accessing substance use disorder treatment options, lack of insurance coverage, legal consequences, stigma, trauma and more.
In this paper, Johnson describes UNC-Chapel Hill’s UNC Horizons program, a treatment program at the UNC School of Medicine with a research-based care model that integrates prenatal care, medication assisted treatment (MAT) and behavioral health services delivered in a trauma-informed environment. This model can improve prenatal care attendance and thus have far-reaching positive implications for both the woman and her newborn child.
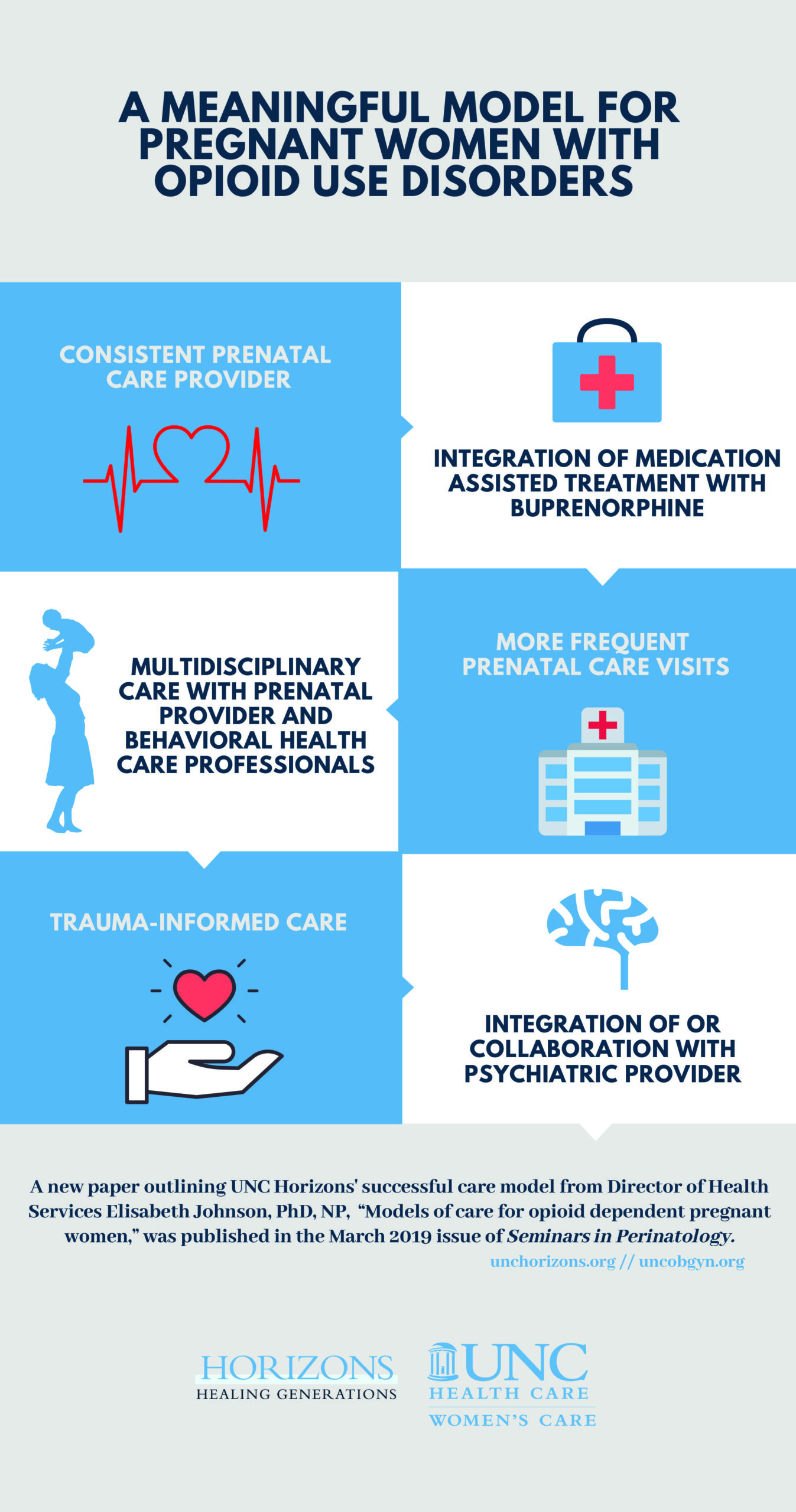
Johnson’s suggested model, like the one at UNC Horizons, contains the following key elements:
- Consistent prenatal care provider
- Integration of medication assisted treatment with prenatal care
- Multidisciplinary care with prenatal provider and behavioral health care professionals
- More frequent prenatal care visits
- Trauma-informed care
- Integration of or collaboration with psychiatric provider
“The obstetrics clinic at UNC Horizons is uniquely situated and able to offer comprehensive integrated care resulting in positive birth outcomes in a high-risk population,” says Johnson. “I want clinics that are not a part of an academic center, and/or do not have direct access to a comprehensive treatment center, to think about ways to create a similar model that fits their practices.”
Given the high rates of opioid use among women in the United States as well as the high rates of unintended pregnancy, it is clear that health care providers need to be prepared to care for the growing population of pregnant women with opioid use disorder.
“Whether or not they are aware of it, most prenatal providers are caring for women who fall somewhere on the spectrum that exists between active substance use and sustained recovery. When we don’t ask, we don’t know and when we don’t know, we are not caring for the whole person.
Johnson says it is important to remember that, with the right models, long-term health is possible. These mothers and their children deserve to heal and recover, she says.
“All the women that I have cared for over the past six years truly want a healthy pregnancy and to be a good mom. Many of these moms are the strongest and most resilient people that I have ever met.”