A Wild Story: Adult Congenital Patient Receives Modified Ross Procedure
Initial Diagnosis
 From the age of 14, Bill Wild knew he had a heart condition. His pediatrician detected a slight heart murmur and sent him in for additional tests. Doctors diagnosed Bill with bicuspid aortic valve, a congenital condition in which the main artery that leads to the body—the aorta—has two cusps instead of three. It is one of the most common congenital heart defects, affecting about 20 per 1000 babies born.
From the age of 14, Bill Wild knew he had a heart condition. His pediatrician detected a slight heart murmur and sent him in for additional tests. Doctors diagnosed Bill with bicuspid aortic valve, a congenital condition in which the main artery that leads to the body—the aorta—has two cusps instead of three. It is one of the most common congenital heart defects, affecting about 20 per 1000 babies born.
Bicuspid aortic valve alone does not cause symptoms in most patients. Over time it may cause the heart’s aortic valve to narrow. This narrowing prevents the valve from opening fully, which reduces or blocks blood flow from the heart to the body. At the time of Bill’s diagnosis, doctors were unconcerned because they did not detect any narrowing of the aorta or issues with blood flow.
 “They told me it was ‘mild’ and wouldn’t stop me from playing sports, which is what I was concerned with since I was just about to enter high school,” Bill recalls. “They said I could do anything I wanted, but I should get it checked out every five years or so and sent me on my way.”
“They told me it was ‘mild’ and wouldn’t stop me from playing sports, which is what I was concerned with since I was just about to enter high school,” Bill recalls. “They said I could do anything I wanted, but I should get it checked out every five years or so and sent me on my way.”
With no immediate action needed, Bill set it aside and did what they suggested, lived his life. He finished high school, graduated college with an accounting degree, got married, had kids, and traveled across the country for work. His multiple roles with Anheuser-Busch took him from St. Louis, Missouri, to California to New York and New Jersey until he eventually landed back in St. Louis in 2012.
At that time, he got a new primary care physician who sent him to a cardiologist to check up on his condition.
“They took a look at the tests and said ‘It’s moderate. It’s narrowed a little, but there are no issues so life is good.’ That was the first time I thought, ‘Oh, that’s different because they had always classified it as mild before.’ But since they weren’t concerned, neither was I.”
 A couple of years later, Bill left Anheuser-Busch and began working for smaller breweries, startups that led to more traveling and additional stress. In 2019 he settled with his wife in Chapel Hill and kept up his on-the-go lifestyle.
A couple of years later, Bill left Anheuser-Busch and began working for smaller breweries, startups that led to more traveling and additional stress. In 2019 he settled with his wife in Chapel Hill and kept up his on-the-go lifestyle.
A Hard Stop
In June 2019, at the age of 42, Bill started to feel uncomfortable pain in his lower body while in Virginia Beach for work. He excused himself from his dinner meeting and went back to his hotel room.
“I was in excruciating pain to the point that I couldn’t stand. I kept thinking this is going to pass, whatever ‘it’ is, it’s got to pass. I waited almost three hours. I was in so much pain I was vomiting. I finally cried uncle at around midnight and headed to the hospital. I walked into the ER, they took one look at me, and immediately diagnosed me with a kidney stone.”
The team performed a CT scan on Bill so they could accurately diagnose the kidney stone. The scan came back and the doctor showed Bill the results. He pointed out the kidney stone on the CT scan which Bill was currently struggling with and they also gave him the heads up that there was another one that would eventually dropdown. The surprising news that Bill also received that day was that he had developed an aortic aneurysm. They told him that it was not at a critical phase yet, but they advised him to get it checked out as soon as he got home.
“I came back and basically ignored it,” Bill said. “It wasn’t until my youngest sister called me; she’s in her last year of residency as a neurosurgeon. She laid into me and made me realize that this is serious, and I need to have it taken care of.”
Starting His Care with UNC
Without a primary care physician on record, Bill had to start the process of beginning his care with UNC. He found a provider and they went through his entire medical history. He received an echocardiogram, which is a graphic outline of the heart’s movement. During an echo test, ultrasound (high-frequency sound waves) from a hand-held wand placed on the chest provides pictures of the heart’s valves and chambers and helps check how the heart’s chambers and valves are pumping blood.
Bill received the results of his tests through the UNCmyChart app on his phone; they were not good. “I look at the results and it says aortic stenosis…severe. My appointment with the cardiologists was a few days away and now I’m freaking out. That’s when I started researching my heart condition.”
Bill met with Elman Frantz, MD, Professor of Pediatrics at UNC and one of the few board-certified adult congenital cardiologists in the state who provides expert diagnosis and treatment for children who have grown up with congenital heart disease and ultimately need treatment in adulthood. Dr. Frantz explained that his heart condition had progressively worsened but he recommended getting a better look at it. Dr. Frantz performed a cardiac catheterization procedure, inserting a long tube into a large blood vessel that leads to the heart. It helps examine how well the heart is working.
Once the procedure was complete, Bill met with John Vavalle, MD, MHS, Assistant Professor of Medicine, Cardiologist, and Medical Director of the UNC Structural Heart Disease Program. After reviewing the results with other experts in the UNC Adult Congenital Heart Program, Dr. Vavalle recommended Bill start planning for surgery sometime in the next six months to a year.
They diagnosed him with aortic stenosis. According to the American Heart Association, it “is the most common and serious valve disease. Aortic stenosis restricts the blood flow from the left ventricle to the aorta and may also affect the pressure in the left atrium.”
Dr. Vavalle also discussed the ascending aortic aneurysm that Bill was initially diagnosed with during his ER visit. According to healthline.com, ”the aorta is the largest blood vessel in the human body. It leaves the heart and forms an arch. The arch’s downward portion, called the descending aorta, is connected to a network of arteries that supply most of the body with oxygen-rich blood. The upward part of the arch, which is the section closest to the heart, is called the ascending aorta. An aneurysm is a bulge that forms in the wall of an artery. It happens when the artery wall weakens. Aneurysms are dangerous because they can rupture and cause massive internal bleeding.”

For Bill, that meant that there was a bulge in his artery in the upward part of the arch in his aorta closest to the heart. “Studies have shown that it’s more common for individuals diagnosed with a bicuspid aortic valve to eventually develop an ascending aortic aneurysm,” says Mahesh Sharma, MD, Chief of Congenital Cardiac Surgery and Co-Director of the NC Children’s Heart Center.
At this point, Bill needed to have heart surgery to correct the defect. He discussed with Dr. Frantz all of the options, including a mechanical valve, a tissue valve, and the Ross procedure.
“I could get a mechanical valve and be on blood thinners for the rest of my life. The longevity of the operation is great. However, dosing of the medicine can be tricky, and as I age, I can see an issue of remembering to take my medication. The tissue valves, on average, last 10 to 20 years depending on how active I am. I want to keep being active, keep working out and maintain a high level of physical fitness. My thought was that if it lasts only 10 years, how many times would I have to go through a transcatheter procedure? I’m going through this at 42 and then again at 52, 62, 72. How many valves can you stick inside of valves before it seems like that’s a bad idea?”
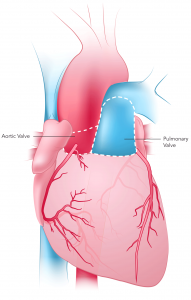
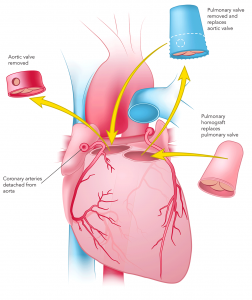
The final option they discussed was the Ross Procedure, a surgery first performed in 1967 in Britain and coined for Dr. Donald Ross. According to the Ross Procedure website, they explain it as “a surgical technique that uses a person’s own healthy pulmonary valve (pulmonary autograft), which is a mirror image of a normal aortic valve, to replace the damaged aortic valve. A donated human pulmonary valve (pulmonary homograft/allograft) is used to replace the pulmonary valve.”
The Ross Procedure (Pulmonary Autograft) (Images from the Ross Procedure Website)
 |
 |
 |
Making a Decision
Bill had a decision to make and he wanted more information. He spoke with doctors in the UNC system and then sought advice from others. Each person he spoke with had a different perspective. “I talked with multiple people and would ask them the same question,” Bill explains. “What would you do if you were me? Each person, from the Chair of Thoracic and Cardiovascular Surgery at Loyola College in Chicago to my baby sister to Dr. Vavalle here at UNC, all said something different. There was no clear answer.”
The final individual Bill spoke with was Dr. Sharma, Surgical Director of the UNC Adult Congenital Heart Program, and someone well-versed in performing operations like the Ross Procedure.
“Bill had done his research, spoke with a variety of physicians, and had a tough decision to make,” says Dr. Sharma. “There is no right answer because they’re all right answers for different people. I couldn’t tell Bill which option he should choose but I did explain to him my extensive experience doing complex congenital surgeries like the Ross procedure. I let him know that whatever option he chose, he would have the highest quality care that UNC could offer.”
The most significant hurdle that they discussed about the Ross procedure is a known complication for adolescent and adult patients. The surgery leads to a risk of late autograft dilation, meaning when the pulmonary valve is under high pressure in the aortic position, over time, it tends to stretch out and dilate and can become an aneurysm again. It can also cause the valve not to work well or develop an insufficiency. Because of that known risk, Dr. Sharma and his team used a modification of the Ross operation. In this modified version, the patient’s autograft pulmonary valve is encased in a Dacron graft before being placed in the patient. All such cases have been successful and shown no risk of dilation after the procedure as of the date of this publication.
 After speaking with Dr. Sharma and weighing his options, Bill decided to move forward with the modified Ross Procedure. On October 9, 2019, he underwent successful heart surgery.
After speaking with Dr. Sharma and weighing his options, Bill decided to move forward with the modified Ross Procedure. On October 9, 2019, he underwent successful heart surgery.
Road to Recovery
Since being discharged from the hospital, Bill has spent his time recovering. Achieving bigger and bigger milestones from first making it up the top of the hill in his neighborhood to now walking six, seven and eight miles a day.
“When we saw Bill for follow-up, it was the best results we could have asked for,” says Dr. Sharma. “His post-operative echocardiogram results were excellent. His heart has good function. Both valves that we replaced, specifically the pulmonary valve that’s in the aortic position, are working flawlessly without any stenosis or regurgitation.”
 Bill is the first to admit that his experience with UNC Health Care wasn’t perfect and he dealt with some hiccups along the way. But overall he was happy with his decision, and it was the right answer for him.
Bill is the first to admit that his experience with UNC Health Care wasn’t perfect and he dealt with some hiccups along the way. But overall he was happy with his decision, and it was the right answer for him.
“I’d never been to UNC before this experience. Then I came in and I ended up with a cardiologist that was specialized in adult congenital cardiology and connected to a surgeon that does a very specific surgery that was useful for someone in my position. All in all, it was a good experience with a very positive outcome. I ended up with the surgery that I wasn’t going to get anywhere else, a surgery that is in my long-term interest. It’s what I wanted and what will support me in the things that I want to do and accomplish in my 40s and 50s.”