Patient Education
Listen to a podcast where Dr. Noone discusses Bronchiectasis
What is Bronchiectasis?
Bronchiectasis is a chronic disease of the lung that can interfere greatly with quality of life in affected individuals. But with proper treatment and monitoring it is possible to improve many of the symptoms associated with bronchiectasis.
The major symptoms include:
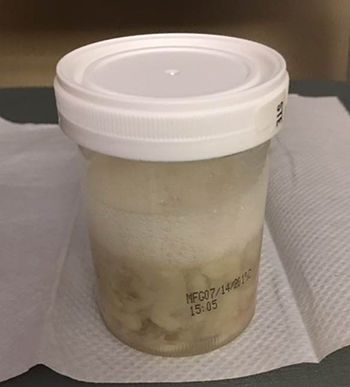
- Cough, usually though not always, productive of green sputum (see Figure 2), sometimes blood
- Shortness of breath
- Other symptoms might include night sweats, fatigue, loss of appetite and weight, and chest pain.
- Symptoms usually wax and wane over time, with periods of relative stability, punctuated by periods of instability (“exacerbations” or flare-ups.)
- Occasionally, and over time, symptoms may be subtle such that patients may carry the diagnosis of asthma, or COPD.
Typically flare-ups, also known as exacerbations, are associated with increased cough, maybe even with coughing up blood, shortness of breath and fatigue. Also known as “exacerbations”, or “flare-ups” these are usually treated with antibiotics: either tablets, or intravenous antibiotics via a “PICC” line, to help reduce the infectious bacteria in the lungs. In adults, it is important to recognize that it is rare to sterilize the airways and lungs completely, even with powerful antibiotics, although these medicines usually greatly improve patient’s well-being by reducing the “burden” of bacteria.
What Causes Bronchiectasis?
The causes of bronchiectasis are varied. Many people have
- Post-infectious bronchiectasis (a prior severe pneumonia for example, or a bad viral bronchitis) or
- Idiopathic bronchiectasis (no cause known)
Some have
- Genetic disease (Primary Ciliary Dyskinesia, or Atypical Cystic Fibrosis)
- Immune deficiency
- Gastro-esophageal reflux disease
- Alpha-1 antitrypsin deficiency
A careful history, physical examination and select tests performed by experts in the field usually provide enough information to make not only a diagnosis of bronchiectasis, but also the likely causes. Some specialized tests for bronchiectasis are only available at expert centers such as UNC. In the case of PCD, nasal nitric oxide measurement and evaluation of the ciliary ultrastructure should occur at a PCD Clinical Center. In the case of CF, sweat testing should be done at a Cystic Fibrosis Foundation Accredited Center. Genetic testing for PCD, and CF may also be appropriate.
What is the Treatment for Bronchiectasis?
Although there is no cure for bronchiectasis, once a diagnosis is established, a program of care can be instituted to plan for significant improvements in quality of life, control of symptoms, a reduction in need for urgent treatments (for “chest infections”, or exacerbations, for example), and most importantly, a reduction in hospitalizations. Often, understanding the nature of bronchiectasis, and knowing that one has expert resources to call on routinely and in times of emergency, is very reassuring and comforting, reducing the stress and anxiety of having a chronic disease..
Why is Bronchiectasis an “Orphan” Disease?
Bronchiectasis had become neglected in recent decades, probably because of the availability of better antibiotics over recent years, the reduction in childhood respiratory illnesses (whooping cough, influenza, pneumonia), and better standards of living. Thus it has become an “orphan” disease in the US and elsewhere, although recent estimates suggest that several hundred thousand in the US are affected with the disease, and the number of patients with bronchiectasis appears to be increasing not only in the US, but the UK, Australia / NZ, and mainland Europe.
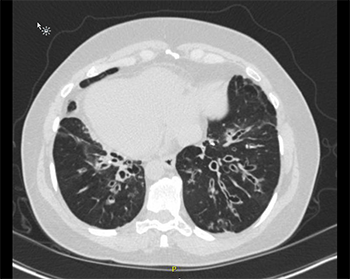
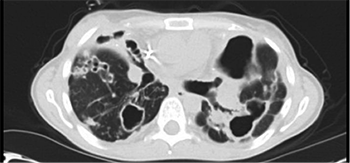
The reasons proposed for the apparent increase in numbers of patients with bronchiectasis range from the increased use of chest computed tomograms (CT), which has increased its detection (see the pictures), to changes in diagnostic labeling (people are often labeled as having COPD, or asthma), to an actual increase in the disease in an aging population
What are Mycobacterial Lung Infections?
Mycobacteria such as Mycobacterium Avium Complex (also known as MAC), or Mycobaterium abscessus are related to the bacteria that cause Tuberculosis (TB), but these “non-tuberculous mycobacteria” (also known as NTM) are very different in the way they infect humans – they are generally not, for example, communicable between humans that we know of. North Carolina appears to have very high rates of NTM, perhaps based on climatic/geographic conditions (humidity, proximity to warm oceanic waters.)
People with pre-existing lung disease (including bronchiectasis) are prone to NTM infections, although occasionally NTM appear to cause bronchiectasis in healthy lungs. Thus, NTM infections and bronchiectasis are closely related in many patients. People often have many of the same symptoms:
- Cough (may or may not be productive)
- Shortness of breath
- Sputum
- Fever
- Loss of appetite and weight
- Abnormal chest x-rays and / or CT scans
How are Mycobacterial Infections Diagnosed?
Patients with bronchiectasis may cough up mycobacteria (MAC for example) without necessarily having significant infection (that is, not necessarily needing treatment) with mycobacteria. Conversely, patients with NTM lung disease almost always have some bronchiectasis on CT scanning. Thus, it requires some expertise to separate which is the dominant problem, and which deserves the most treatment, at least initially. This is important because of the implications of treatment of mycobacteria – it is very time intensive, and can be very onerous to patients (sometimes years of systemic drugs.)
Diagnosis of NTM infection in the lungs requires sputum cultures, specifically AFB sputum cultures. These cultures can take up to 6 weeks to be finalized because the bacteria can take a long time to grow, particularly MAC. The slow growth is why treatment duration is long but it also provides the opportunity for us to think carefully about the right treatment for you.
Good clinical care of people with mycobacterial lung infections requires experienced clinicians, with good teamwork, hence the creation of the UNC Center for Bronchiectasis Care. NTM lung disease shares many clinical characteristics with bronchiectasis; patients tend to be older, female, with deleterious effects on quality of life, and demanding of rigorous, longitudinal treatment schedules, while carrying a high commitment of time and energy and a financial health care cost. While there is not that much research information to guide evidenced based diagnosis and care, nonetheless experts in the disease can successfully manage it to achieve good outcomes in most cases.
At UNC, there exist several physicians interested in both bronchiectasis and mycobacterial lung infections / NTM, such that we will strive to give all patients the very best possible attention and care.
Primary Ciliary Dyskinesia:
What is PCD?
Primary ciliary dyskinesia (PCD) is an umbrella term for inherited (genetic) disorders of microscopic, little hairs called cilia that line the upper and lower respiratory tract including nasal passages, sinuses and lung, and Eustachian tubes of the ear, the reproductive organs, and the ventricles of the brain. The activity of motile (moving) cilia, working in cooperation with airway mucus, provides a first line of defense for the airways, maintaining healthy airway tissue. This important biological system is known as ‘mucociliary clearance.’ Defects of mucociliary clearance can lead to profound illness.
What are some of the features of PCD?
With rare exceptions, people with PCD exhibit the following symptoms:
- Respiratory problems in the newborn period despite full term birth
- Daily, year-round, wet cough starting in the first year of life (usually first months of life) that does not go away with change of seasons. It may improve with antibiotic treatment, but never fully resolves
- Daily, year-round nasal congestion starting in the first year of year of life (usually first months of life) that does not go away with change of seasons
- Any laterality/situs (organ placement) anomaly and/or organ development issue, plus the above
In older children and adults, all of the above remain constant, plus:
- Development of chronic otitis media with effusion and/or recurrent ear infections
- Development of chronic pansinusitis (all sinuses involved)
- Bronchiectasis on chest CT scan or x-ray (all adults with PCD have bronchiectasis)
- Fertility issues (Male infertility, female sub-fertility or ectopic pregnancy)
How is PCD Diagnosed?
Diagnosis of PCD presents a number of challenges and can often be a complex process. There is no single diagnostic testing option that is 100% effective.
Most importantly, there is a strong clinical phenotype—or physical presentation—associated with PCD (see above). Diagnostic testing performed in the absence of this presentation is not recommended, as it has led to an unacceptably high rate of false positive diagnoses in PCD (people being told they have the disorder when they do not).
Nasal nitric oxide measurement can be used as a screening tool to determine whether PCD is a likely diagnosis. This test is not approved for diagnosis in the United States at this time and is primarily used in the research setting. Confirmatory testing is needed to formally diagnose PCD. These include:
- Biopsy of ciliated tissue (usually from the nose or trachea) with analysis of ciliary ultrastructure. This biopsy should be done and evaluated at a PCD Clinical Center and when the patient is feeling well. This helps minimize the possibility of changes that are not caused by genetic mutations being classified as caused by PCD.
- Genetic test showing two mutations known to cause PCD—one from each parent
How is PCD Treated?
In 2015, PCD experts from North America, including top pulmonologists, medical professionals, and PCDF representatives published recommendations for diagnosis, monitoring, and treatment of primary ciliary dyskinesia. This consensus statement represents the best evidence currently available from expert physicians and researchers with years of experience diagnosing and treating PCD. It will be periodically updated as the evidence directs. Please feel free to download and share with your own physicians.
Airway Clearance
What is airway clearance?
Airway clearance is how we move mucus out of the airways. In bronchiectasis and NTM infection, there is impaired clearance of the mucus, regardless of the cause. When mucus sits in your airways, it causes inflammation and possibly further damage to your lungs. Mucus also holds bacteria within your airways, leading to more inflammation and recurrent exacerbations. Because of this, it is critical to improve your airway clearance to get the mucus out of your airways.
What are the options for airway clearance?
- Active Cycle Breathing Technique: Three phases of breathing techniques that help make your cough clearance even more effective. Help to relax the airways, then get air behind mucus to clear it, followed by forcing the mucus out of your lungs.
- Exercise: 20 to 30 minutes of aerobic activity of your choice. This includes Zumba classes, jumping on a trampoline, swimming, etc.
- Pros: Can be inexpensive and exercise has other benefits like improving bone density, mood, and overall health
- Cons: May not feel like exercising when you are sick or when the weather is bad. If you haven’t been exercising, it might be hard to know where to start. In this case, pulmonary rehab might be right for you.
- Nebulizing hypertonic saline: Using a nebulizer to inhale sodium chloride 3% or higher concentrations helps pull water into the dried mucus in the airways, making it easier to dislodge it and cough it out. It is also a little irritating to the airways so it can make your cough more forceful.
- Pros: Treatments typically take 10 minutes and are very easy to do. Lots of patients find it very effective.
- Cons: Some insurance companies don’t cover sodium chloride. Some people may need to use albuterol before or with the hypertonic saline because it can make airways twitchy and narrow. You need a nebulizer and to clean the nebulizer cups.
- Hand-held PEP devices: Examples include: the Acapella Choice®, the flutter valve, the Pari-PEP, and the Aerobika. You steadily blow out through the device, which produces a flutter sound and wave. This flutter wave is conducted down your airways to help shake and shear the mucus off your airway walls. The flutter wave also keeps the airways open when you breath out so that you have more room to move the mucus out. Some of these devices allow you to nebulize through them at the same time.
- Pros: Small and portable. Pretty easy to get these devices (often through a durable medical equipment [DME] company).
- Cons: Cleaning is still necessary. Insurance coverage of each device varies. Some devices are not carried by DME companies.
- Percussion vest: There several companies who make these devices and the choice of which Vest depends on what features are important to you and your doctor. Vests are typically worn for 20 to 30 minutes per day, and provide pressure waves around your chest. These waves are transmitted to your airways to help shake and shear the mucus off your airway walls.
- Pros: Can be worn while nebulizing. Effort independent, meaning that the vest will provide these vibrations even when you are sick or even asleep. Minimal cleaning
- Cons: Expensive – insurance requires that you have failed other airway clearance methods. Bulky so difficult to take on trips, although there are now portable versions.
- Postural drainage: With postural drainage, you get into a position that helps drain fluid out of the lung. Because the airways of the lung branch out in different directions, mucus drainage from the upper portions happens because of gravity. Mucus doesn’t drain well from the lower lobes because it would have to move up-hill.
- Pros: Can be done as part of a yoga or Pilates class. Inexpensive.
- Cons: Do not perform right after a meal or if you have GI issues like delayed gastric emptying, gastroparesis, or severe GERD (reflux).
- Chest physiotherapy: Either you or someone else claps a hand or a cup-device over your ribs and back, spending 5 to 7 minutes on each area of the chest. This helps shake the mucus off the airway walls and is often done in conjunction with postural drainage.
- Pros: Inexpensive. If done by someone else, method is effort-independent.
- Cons: Can be hard to reach your back if you are doing it. Need a caregiver who is around to perform therapy and is willing to dedicate time to doing it properly.
What method is the best?
The best method is the one that works for you. If you find it effective, you are more likely to do it. If it fits into your life, you are more likely to do it. We don’t have studies that show that one device or method is better than another method or device. As you can see, there are pros and cons to each method. You may find that you want to use one device when you are well and another when you are sick. You may want to use several devices at the same time, like nebulizing hypertonic saline through a PEP device or performing postural drainage while wearing the vest.
Does this mean I’ll cough up more sputum?
Not necessarily. We notice if we cough up big globs of sputum but if the sputum is broken in to small pieces, they are swept up the airway and swallowed without us paying much attention. Some patients find that when they regularly do airway clearance, they don’t cough up much sputum. If the amount of sputum doesn’t decrease, you are still getting benefit from doing the therapy. Remember that for all of the mucus you’ve seen coming up from your lungs, there is more in there that hasn’t come up, at least not until we help it come up. The measure of how well airway clearance is working is not sputum production. Rather, it is improvement in lung function, decrease in exacerbation number and severity, chest feels less congested.
How often do I need to do airway clearance?
Think of airway clearance as bronchial hygiene. Like dental hygiene, we recommend performing bronchial hygiene at least twice a day: in the morning and in the evening. When you perform clearance in the morning, you are moving out the mucus and secretions that have settled in your airways overnight so you can start the day off right. When you perform clearance in the evening, you are clearing out the irritants, particles, and mucus that you inhaled during the day, allowing you to get more restful sleep.
When you are sick with an exacerbation, or an acute worsening of your lung disease, you have more mucus that needs to be cleared out of your airways. You should increase your airway clearance frequency to make up for this. Even if you are on antibiotics, it is still very important to perform your airway clearance. By moving the mucus out of your lungs, the environment is not as friendly to the bacteria, making it harder for them to stick around.
How do I clean my equipment and how often?
Nebulizer cups and hand-held airway clearance devices need to be cleaned with warm soapy sterile water after each use. Additionally, the cups and hand-held devices should be sterilized daily. Options for sterilization may vary by device but typically include boiling for 5 minutes, soaking in rubbing alcohol (70% isopropyl alcohol) for 5 minutes and rinse with sterile water, or using a baby bottle sterilizer. We do not recommend using vinegar to clean your equipment because many of bronchiectasis patients have bacteria that are not killed using vinegar. To prevent bacteria from growing on your equipment (and then inhaling the bacteria), it is important to clean and sterilize your equipment daily. Reusable nebulizer cups and the tubing should be replaced by the DME company every 6 months. Do not wash or boil your nebulizer tubing. Disposable nebulizer cups will melt in high heat so be sure to ask your DME company for reusable cups.
UNC Research in Bronchiectasis
The staff of the UNC Center for Bronchiectasis Care have been heavily involved in research into the causes and treatment of bronchiectasis in its many forms for decades. In the early 1980s, Drs Richard Boucher and Michael Knowles began ground-breaking work into the causes of cystic fibrosis at a very basic level, which led quickly to a clinical studies of new therapies. This set the stage for many clinical trials of investigational therapies over the ensuing years, with Drs Noone and Knowles studying new treatments for CF and Primary Ciliary Dyskinesia throughout the 1990’s and the 2000’s. The studies were often partnered with local funding sources, the NIH, the Cystic Fibrosis Foundation, and Industry.
More recently, the Care Team has partnered with Industry to help study new treatments for non-CF Bronchiectasis and NTM, most often in the form of new preparations of inhaled antibiotics and mucus thinning / airway hydration treatments.
Two such studies of specially formulated ciprofloxacin for inhalation have finished enrollment, and another studying the safety and effectiveness of VX-371 in patients with PCD is ongoing. We expect many such studies of new therapies for bronchiectasis and NTM to come on stream over the next few years. We also have “in-house” studies addressing various aspects of the pathogenesis and treatment of the diseases. More information on research studies can be found at clinical trials.gov.
Finally, as previously mentioned, UNC is a founding partner of the US Bronchiectasis Registry, which is rapidly evolving throughout the US to involve more and more researchers and sites, and now includes NTM initiatives. Annual meetings with our international collaborators have commenced in Europe and North America to exchange knowledge and ideas.
Links:
General Education about Bronchiectasis:
- The American Lung Association: Bronchiectasis
- Patient Guide from the British Lung Foundation
- Bronchiectasis Toolbox from the Thoracic Society of Australia and New Zealand
- We note the recent development of “BronchandNTM360social” which is a global, online community for individuals affected by Bronchiectasis and/or NTM, including patients, family members, caregivers, physicians and other healthcare providers. It serves as an online home for these communities and provides a comfortable venue to share thoughts and ideas, ask questions, start discussions, read and comment on blogs, and communicate with peers, thought leaders and community managers. BronchandNTM360social is part of the Bronchiectasis and NTM Initiative, which aims at meeting the unmet needs of the Bronchiectasis and NTM communities. Along with BronchandNTM360social, the Initiative offers educational resources for patients and research programs meant to assist in accelerating therapeutic solutions and cures for both, Bronchiectasis and NTM.
Known Causes of Bronchiectasis:
- Cystic Fibrosis Foundation: www.cff.org
- The Primary Ciliary Dyskinesia Foundation: https://pcdfoundation.org
- NTM Info and Research, Inc.: https://www.ntminfo.org
- Alpha-1 Foundation: https://www.alpha1.org/what-is-alpha1
- Immune Deficiency Foundation: https://www.primaryimmune.org
Research:
- UNC Marsico Lung Institute: https://www.med.unc.edu/marsicolunginstitute
- Interested in clinical trials and other research opportunities? www.clinicaltrials.gov